
Quality Matters: From Insight to Impact
Before solving a problem, you must first understand it

Quality Improvement (QI) is critical to delivering on the NHS Plan. This series of articles from Associate Directors, Ian and Laura, provides a personal and practical insight into how QI is needed more than ever.
Veran Patel, Director, Health & Social Care
One of the things that is striking about our quality improvement work in healthcare is that most of the time the problem as presented, the one we were asked to help solve, wasn’t really the problem at all. Now, you may well be thinking, ‘that isn’t us!’ and maybe you are right. Our counter would be that in the majority of situations we come across, people generally think they have a good handle on issues and the corrective action required to fix them …. yet here we are.
There might be further anecdotal evidence that supports our premise. A general theme raised by many staff in organisations we have supported is a sense that their leaders often ‘jump to solutions’ and perhaps more than that, those solutions do not resolve the issue at hand; worse still, they may make matters more complicated, disempower staff, impact morale and further degrade service.
So, why might this happen and what can we do to prevent it? Well, the reason it happens is wide-ranging and, in our experience, might include one or more of the following:
- Inaccurate or misinterpreted data. Organisations have great volumes of data at their disposal, reems of data definition and they deploy significant time and resource entering, analysing and reporting data. Yet we always find error in it and sometimes that error is sufficiently significant it can mislead a Board into taking action and making decisions it would not otherwise consider; one Board set up a whole programme of work based on erroneous data. We become most sceptical when people outline a problem and talk of benchmarking and/or outliers; each time someone has told us they were an outlier, we went on to discover they were not.
- Poor diagnosis of root cause. When I joined the NHS in 2005, I sat next to a patient safety team collating and analysing serious untoward incidents. For each one, the apparent outcome was that someone needed to be disciplined and/or re-trained. I recall mentioning human factors and FMEA at that time to be greeted by blank looks. Things have improved greatly since, at least in the domain of patient safety, but we do not see much rigour in the root cause analysis of poor-performing systems and processes.
- Pre-conceived or knee-jerk solutions. I have sat in management meetings and watched people present a concern, with solutions proposed almost immediately and people quickly voicing support. A decision is made, outline plan agreed. Such is the speed of arriving at a solution, one cannot help thinking it was either ‘the first thing we thought of’ or something that was waiting in the wings for a suitable problem to announce its cue.
- Bias towards simple and convenient answers to complex problems. Equally I watch people present complex, multifactorial problems that are very hard to understand and hold fully in one’s head, and see that reduced to simple cause and effect relationships, with confidence that doing one thing will lead to successful resolution. By definition, complexity does not usually behave in simple ways so there is high risk the solution will not be successful – worse, it might shift performance in the opposite direction and/or create all manner of unintended consequences, with people not necessarily aware that it is their solution that has created them. We often see solutions layered over each other, like wallpaper over wallpaper. In time you can lose sight of the core of what you are seeking to achieve.
- Direction from above to do something specific, expeditiously. Maybe this is the mother of all of the above, with a solution that may well have merit in the place in which it originated, for reasons specific to that place, being foisted on other organisations and services from on high, perhaps with genuine belief (or hope) that improved outputs and outcomes will be similarly realised. I don’t see any wholesale evidence that this approach works.
To prevent such scenarios playing out we need to shift focus, effort and resource to fully understanding a problem, and away from contriving solutions… there is a relatable Einstein quote in there somewhere. This of course aligns well with intent expressed by NHS Impact that leaders become problem-framers, not problem-solvers. In our 5-step improvement approach below, it is in Steps 1 and 2 that we seek to fully understand a problem, before contemplating solutions.
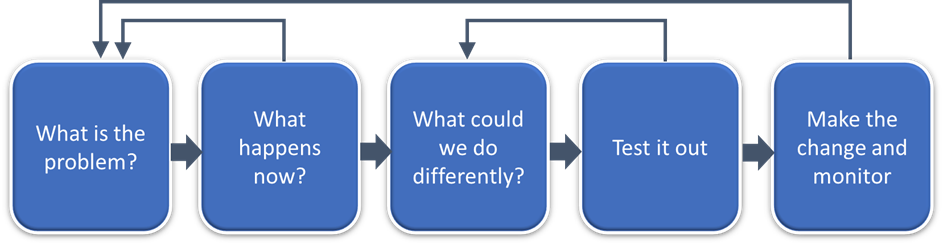
Figure 1: Our 5-step improvement approach
In Step 1 we ask, ‘what is the problem you are trying to solve?’. In our experience people often express ‘the problem’ as a need to implement a stated solution, or the need for some key people to ‘get onboard’ with that solution. Those solutions typically focus on a perceived, but not necessarily evident root cause, perhaps with a smattering of ‘we need more resource’ or ‘the fault lies elsewhere’. We tend to answer such responses with ‘that sounds like a solution, so what is it a solution to?’. Some time later we get to a relatively straightforward answer to Step 1, a problem typically expressed as a single sentence, identifying at least one key metric causing issue e.g. ‘ambulance handover at ED is below target with 47% complete within 15 minutes’ or ‘the % of colorectal cancer patients starting treatment within 62 days of referral is below target at 69%” or “15% of adult MH inpatient admissions had been discharged from an inpatient ward less than 30 days prior”. The beauty of these problem statements is that they focus on the issue and invoke curiosity to explore: is that right? why is that? what is causing it? In short, the problem has been framed, not solved.
In Step 2 we seek to understand in detail ‘what happens now?’ because whatever is happening now is surely driving the issue at hand. We want to know the systems and processes involved, where they start and finish, what happens before, after and in every step between. We want to know demand and capacity, how long tasks take to do and what people, skills and equipment are required. We want to understand different flows, especially of information, patients, staff and equipment. We want to understand error rates, re-work, workarounds, complaints. We want to know the experience of staff and of customers (typically patients and carers) of the service. In doing all of this we want to keep the scope as wide as possible for as long as possible, accepting this means more work but recognising that root cause does not always reside where symptoms manifest.
Critically, to fully understand the detail of ‘what happens now’ in Step 2, we explore 3 separate perspectives: what system data reports happens; what people say happens; what we see happening by observing work for ourselves – the latter is almost always the most powerful so while it also takes more time and effort it is usually a false economy to curtail it.
As we go through Steps 1 and 2, we iterate. The more we understand about what happens now, the better we understand and more able we are to refine the problem statement and close in on root cause. By the time we get to Step 3 the problem and its potential solutions are far more obvious, especially to staff and patients who work and use the service. Crucially, people buy into solutions they have designed, solutions which are typically far better, more innovative and cost effective than those originally proposed.
It has taken time to get here (maybe 8-10 weeks) but now we can expedite testing and implementation of solutions we are confident will be successful. At the start, some leaders will say we do not have time to do this work and must act now – we say, ‘understanding a problem is acting now’. What we never hear a leader say at the end, is ‘well this is the solution we were going to do anyway’ – that has never happened!
Laura Woodward and Ian Railton are Quality Improvement (QI) experts and are Associate Directors at TIAA. This series of fortnightly blogs are their insights into a long career and successful track record of working with healthcare organisation to improve productivity and better outcomes for patients.

